Sarcopenia
Please remember the advice we give is general and not meant to be used as a substitute for professional medical or health advice, diagnosis, or treatment. If you want specific advice then please seek help from your doctor or local physio.
Muscle mass and ageing
Anabolism is the process of building up tissues such as muscle. As we get older, our bodies become anabolically resistant. Hormonal changes during ageing makes it much harder to retain or build muscle tissue. Anabolic resistance is hardest hitting for those who are largely sedentary. This is because physical activity, in particular resistance training, is one of the best ways to build and retain muscle! Physically inactive adults lose around 3-8% of their muscle mass per decade after the age of 30, and this process accelerates after age 50. So a sedentary person at age 80 can expect to have lost around 40-50% of the muscle mass they had at age 20 (2). Such a large decline in muscle mass will lead to many sedentary older adults being diagnosed with sarcopenia.
What is sarcopenia?
Sarcopenia comes from the ancient Greek for ‘a poverty of flesh’. People with sarcopenia have severely reduced muscle mass and strength, to the point where they have trouble with everyday tasks. It is NOT a normal part of aging but is more prevalent than you might think. Sarcopenia is diagnosed based on these three criteria:
- Low muscle strength - you may have difficulty with everyday tasks such as standing from a chair or climbing stairs.
- Low muscle mass - a health professional can identify whether you have a significant deficit in muscle tissue quantity simply by observation. This can be more accurately measured via DXA scan, however this is not required.
- Poor physical performance - a physiotherapist can identify this using tests such as a 5x sit-to-stand test where we measure how long it takes to rise from a chair 5 times.
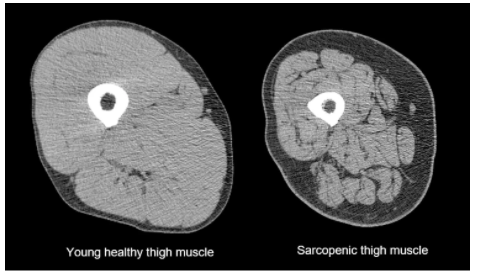
Another feature of sarcopenia is ‘marbling’. This is fat infiltration in and around muscle fibres and is a marker of low muscle tissue quality. Muscles with a high degree of fat infiltration are less healthy, and tend to be less effective at producing force.
What causes sarcopenia?
We have seen that older adults naturally lose a lot of muscle mass over their adult years, but it is the imbalance of factors that cause muscle breakdown (catabolic) over factors that cause muscle build up (anabolic) that cause someone to become so anabolically resistant that they develop sarcopenia. Some of these factors are outlined in the table below.
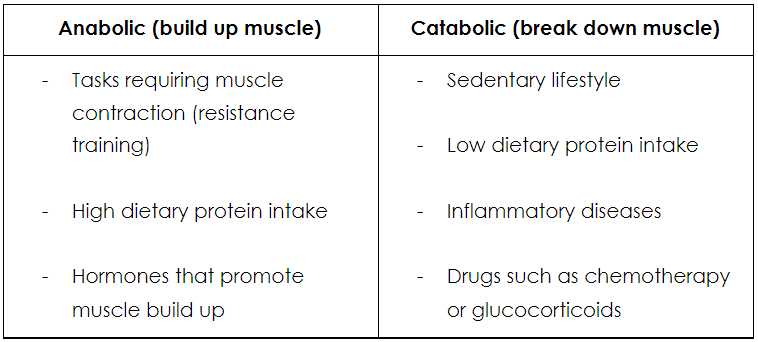 Table 1: Anabolic and catabolic factors of sarcopenia (2)
Table 1: Anabolic and catabolic factors of sarcopenia (2)
Why is it important to avoid sarcopenia?
First and foremost sarcopenia takes a massive toll on an individual’s functional capacity. This is the pool of energy that a person has to give to each of their everyday tasks - if getting out of a chair is a maximal effort, the task will take a lot more out of someone than those who find it easy. The same can be said for showering, cleaning, cooking, doing the groceries, playing with children…. the list goes on!
The other big impact of sarcopenia is on our physiological reserve. This is the "physical superannuation" or "money in the bank" that we keep for tough times. When someone is hospitalised due to an injury or illness, they tend to lose muscle mass and strength. If someone is sarcopenic, they only have to lose a very small amount to lose what independence they had left - making it much more likely that they will be discharged to a care facility rather than their own home.
In addition, sarcopenia is a strong indicator of all-cause, cardiovascular and cancer mortality, so clearly losing muscle mass is something we should all be trying to avoid.
What can you do to avoid sarcopenia?
To prevent or treat sarcopenia, we need to increase the anabolic factors relative to the catabolic ones, as per table 1! Importantly, we need to increase the amount of muscle stimulating contractions (resistance training) and increase the dietary intake of protein in order to supply the muscles with the building blocks to create muscle tissue. Resistance training should meet or exceed the minimum physical activity guidelines of at least 2 strength based sessions per week, challenging all the major muscle groups through a full range of motion. However, the dosage is important and should be individualised on a person-by-person basis. The evidence suggests that higher exercise volumes show a greater muscle synthesis in those with sarcopenia than lower volumes. For example, doing 4 sets of squats will likely provide a greater response than performing 2 sets.
This principle of greater dosage applies to dietary protein too. The evidence suggests that older adults should consume between 1.2-1.6g per kg of lean body weight, per day, in order to maximise muscle protein synthesis. So a 60kg person should be aiming to consume between 72 and 96g of protein each day. This can take a variety of forms depending on the person’s personal preference (see table 2 for ideas!) This is far greater than the recommended dietary intake of 0.8g per kg of bodyweight, but has been shown to be safe in healthy individuals. (Note: a more rigorous cost-benefit analysis of protein intake should be undertaken in those with chronic kidney disease who are sarcopenic.)
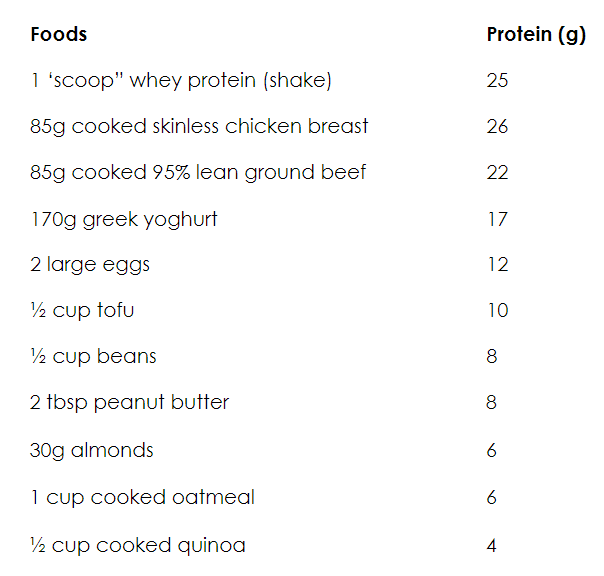 Table 2: Protein content of various foods
Table 2: Protein content of various foods
Summary
We have seen that sarcopenia is a severe loss of muscle mass, strength and function, resulting in increased risk of hospitalisation, mortality and loss of independence. Thankfully you can maintain and build muscle mass with sufficient resistance training and dietary protein intake!
And remember… if you don’t use it, you lose it!
References
- Anderson, R., & Kenney, W. (2021). Effect of age on heat-activated sweat gland density and flow during exercise in dry heat | Journal of Applied Physiology. Journal of Applied Physiology. Retrieved 29 November 2021, from https://journals.physiology.org/doi/abs/10.1152/jappl.1987.63.3.1089.
- Baraki, A. (2021). Sarcopenia Lecture w/ Dr. Austin Baraki. Youtube.com. Retrieved 29 November 2021, from https://www.youtube.com/watch?v=wJBqBDZoSvQ.
- Stephen Thielke, M. (2021). Aging: Are these 4 pain myths complicating care?. PubMed Central (PMC). Retrieved 29 November 2021, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4356472/.
- Trompeter, S., Bettencourt, R., & Barrett-Connor, E. (2012). Sexual Activity and Satisfaction in Healthy Community-dwelling Older Women. The American Journal Of Medicine, 125(1), 37-43.e1. https://doi.org/10.1016/j.amjmed.2011.07.036